Revision Rhinoplasty
Revision rhinoplasty strives to allow the patient to attain a greater sense of satisfaction with their desired outcomes
CUSTOMISED PLAN FOR REVISION RHINOPLASTY
We have a solution for every complication
Rhinoplasty Materials
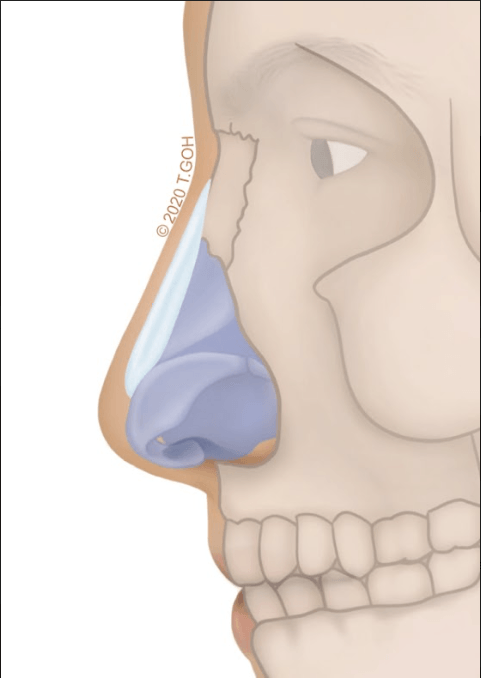
Silicone | Goretex
Silicone has been the commonest and oldest implant for rhinoplasty. It does not get absorbed and keeps its shape even after a long time. It is great for creating the curved lines. Adequate skin cover is necessary for safe use of silicone implants. Capsular contracture can lead to short nose.
Gore-tex easily assimilates well with natural tissue due to its porous nature. Its soft texture enables it to be used in patients with then skin and it looks very natural after an operation. However it is harder to remove and may become lower due to tissue integration.
Diced Cartilage + Glue | Fascia
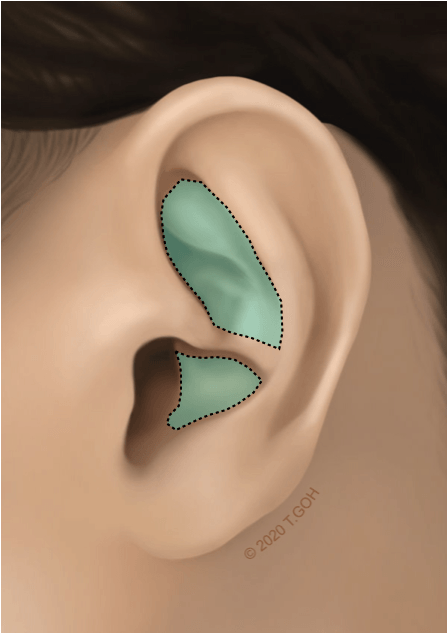
Diced Cartilage + Glue. Finely diced cartilage is mixed with tissue glue to create a bioactive paste which can be use to smoothen minor irregularities or create a mild elevation of the dorsum. The cartilage can be taken from the septum or ear cartialge. Due to resorption, there may be some loss of dorsal height.
Diced Cartilage + Fascia. The diced cartilage is wrapped within fascia harvested from the scalp through a hidden incision. Economical use of the cartilage enables the surgeon to maximise the cartilage to create full dorsal augmentation. Resorption rates are low as the diced cartilage is wrapped within the fascia. Irregularities and deviation are also uncommon.
Fascia only. Fasica only grafts can be used to augment the radix or to increase the thickness of noses with very thin skin.
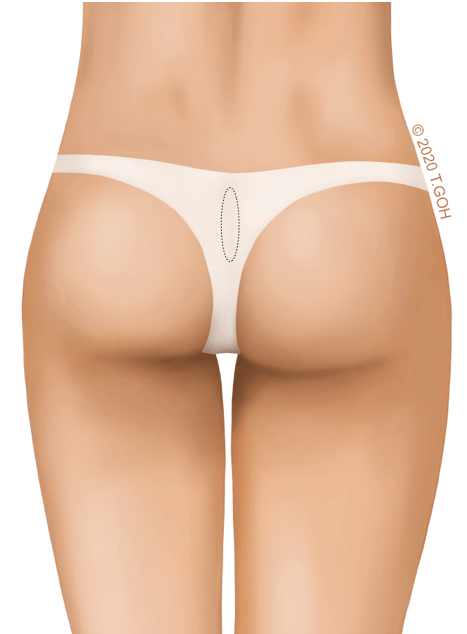
Dermatofat Graft
Dermal grafts can be taken from anywhere in the body. The back of the buttock is an ideal place for a well-hidden scar. The skin and fat can be used to augment the nose for a natural look without implants. There is however a 20-30% resorption rate.
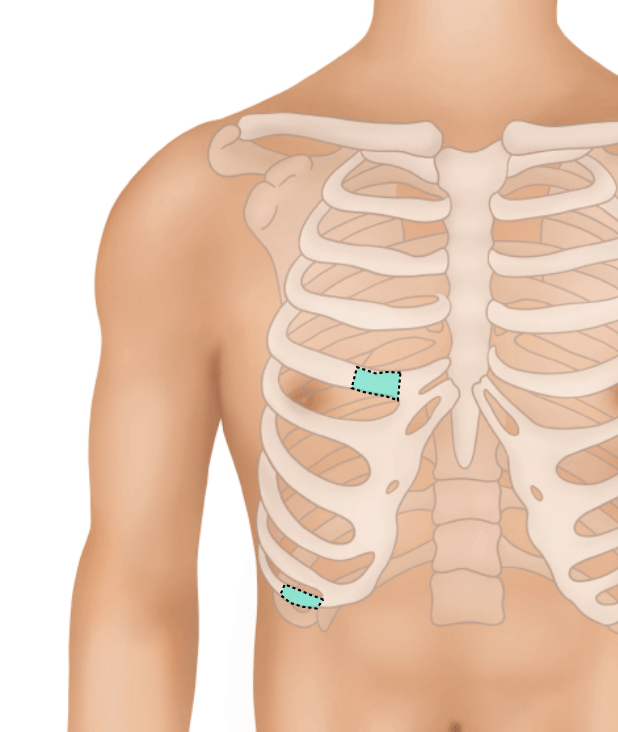
Gold standard
The rib presents a large volume of cartilage which can be used en-bloc or diced and placed within fascia. Enbloc rib cartilage is used mainly in reconstructive surgery where large volume of cartilage is required and diced cartilage is preferred for augmentation. The rib is a versatile donor site but rib surgery requires overnight stay and is the most expensive option.
Getting Revision Rhinoplasty Right
01
Diagnosis
02
Autologous Rhinoplasty
03
Considering facial angles and proportions
Hospitalisation
Anaesthesia
Operation Time
Removal of Sutures
RELATED PROCEDURES

TIP-PLASTY

ALAR-PLASTY
